Notice first symptoms – how to recognize liver disease
Do you think that a friend or family member might have a liver disease? Or has a friend or family member of yours recently been diagno... | more
Liver Diseases

Hepatic encephalopathy (HE) is a liver-related brain dysfunction. The term comes from Greek and means „disease of the brain caused by the liver“. It comprises all disorders of brain function that are associated with acute or chronic liver diseases (e.g. liver cirrhosis). The disorders of the brain occur because the liver is too damaged to detoxify the body. HE is often a chronic disease, i.e. the disease persists as long as it is not treated.
Several processes in the body are involved in HE. In particular, the affected liver can no longer ensure sufficient ammonia detoxification. Ammonia is produced by metabolic processes mainly in the intestines, muscles and kidneys, e.g. in the digestion of dietary proteins. If the liver no longer works sufficiently, ammonia enters the brain via the bloodstream. That leads to an increasing poisoning and as a consequence to the disturbance of the brain function and change of mental state.
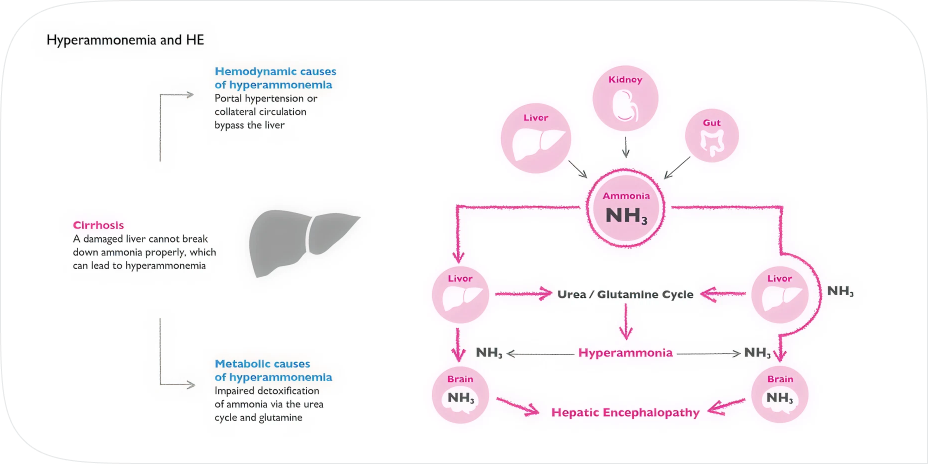
Ammonia is toxic to the brain. When ammonia levels are raised – this is also described as hyperammonemia – brain functions such as concentration and memory are disturbed, mood worsens, fatigue and weakness appear. All of this can severely impair the quality of life and even be life-threatening in cases where increased concentration is required.
When ammonia levels are reduced, these problems are eliminated and the condition is normalized.
Elevated ammonia attacks liver cells, which leads to the progression of the disease: the blood circulation inside the liver is disturbed and the liver’s ability to recover is reduced. Over time, the cleaning function of the liver is disturbed even more as the level of ammonia continues to grow.
The negative effect of ammonia is reversible – reducing the level of ammonia protects the liver and improves its condition.
Elevated ammonia in the blood has a negative effect on muscles, resulting in a reduction in muscle mass, muscle strength and increased muscle fatigue. It also leads to slower recovery from sports training and fatigue.
The symptoms of hepatic encephalopathy (HE) vary depending on the stage of the disease. They range from comparatively mild symptoms such as sleep and concentration disorders, personality changes and disturbances of consciousness to life-threatening liver coma.
Even the initial stage of HE (covert hepatic encephalopathy, CHE) with its comparatively harmless symptoms should be taken very seriously. The symptoms of covert HE are already detectable in about 60-70% of all patients with liver cirrhosis.
The symptoms indicate that further medical clarification and treatment are urgently needed to prevent the disease from progressing. A covert HE already leads to diminished attention, reaction and concentration ability, which can also result in limited driving ability. HE is classified according to the so-called „West-Haven criteria“ into four degrees of severity plus the preliminary stage of minimal HE (MHE). Classification is mainly based on the mental state of the patient.
An early diagnosis is important: The earlier HE is diagnosed and treated, the less the disease can progress and the better the symptoms, quality of life and general condition of the patient can be controlled.
Chronic liver disease: Experts assume that chronic liver diseases such as fatty liver disease or cirrhosis of the liver very often lead to HE. Since HE is always based on liver disease, both liver disease and HE must be diagnosed.
Clinical symptoms: Clinical symptoms are an important basis for the diagnosis of HE. This refers to symptoms that can be recognized from the outside and described by the patient and their relatives, such as fatigue, tremors, reduced ability to react. The severity of HE is also determined on the basis of these symptoms.
Psychometric tests: So-called psychometric tests have proved their value in determining mental condition such as concentration and fine motor skills more precisely. One example is a so-called “Number Connection Test” which you can do on this website.
Neurological examinations: In addition, neurological examinations such as critical flicker frequency analysis (CFF) or electroencephalography (EEG) can be performed in clinics or specialized liver centers.
Blood tests: Blood tests are not a priority for the diagnosis of HE. The determination of blood ammonia is rather difficult and is associated with sources of error (sample must be cooled immediately until analysis). However, they are very helpful for diagnosis and follow-up of the underlying liver disease.
According to ISHEN classification, today covert and overt HE are characterized by specific West-Haven criteria combinations as summarized below.
| WHC,including MHE | ISHEN | Description | Suggested operative criteria | Comment |
|---|---|---|---|---|
Unimpaired |
No encephalopathy at all, no history of HE |
Tested and proved to be normal |
||
Minimal |
Covert |
Psychometric or neuropsychological alterations of tests exploring psychomotor speed/executive functions or neurophysiological alterations without clinical evidence of mental change |
Abnormal results of established psychometric or neuropsychological tests without clinical manifestations |
No universal criteria for diagnosis. Local standards and expertise required |
Grade I |
Covert |
• Trivial lack of awareness • Euphoria or anxiety • Shortened attention span • Impairment of addition or subtraction |
Despite oriented in time and space (see below), the patient appears to have some cognitive/behavioural decay with respect to his/her standard on clinical examination, or to the caregivers |
Clinical findings usually not reproducible |
Grade II |
Overt |
• Lethargy or apathy • Disorientation for time • Obvious personality change • Inappropriate behavior |
Disoriented for time (at least three of the followings are wrong: day of the month, day of the week, month, season, year) +/- the other mentioned symptoms |
Clinical findings variable but reproducible to some extent |
Grade III |
Overt |
• Somnolence to semi-stupor • Responsive to stimuli • Confused • Gross disorientation • Bizarre behavior |
Disoriented also for space (at least three of the following wrongly reported: Country, State -or region-, city, place, +/- the other mentioned symptoms |
Clinical findings reproducible to some extent |
Grade IV |
Overt |
Coma |
Do not respond even to pain stimuli |
Comatose state usually reproducible |
Weissenborn K. Hepatic Encephalopathy: Definition, Clinical Grading and Diagnostic Principles. Drugs. 2019 Feb;79(Suppl 1):5-9. doi: 10.1007/s40265-018-1018-z.
Table reproduced from Vilstrup H, Amodio P, Bajaj J, Cordoba J, Ferenci P, Mullen KD, et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology. 2014;60:715–35.
Main goal: reduction of increased ammonia concentration in the blood
The main aim of HE therapy is to render the ammonia in the body harmless before it reaches the brain, irrespective of the underlying liver disease.
Increase in ammonia detoxification in the liver – ammonia is collected regardless of where it originates.
Reduction of ammonia production and absorption from the intestine. Only the ammonia produced in the intestine is collected.
As long as an underlying advanced liver disease is present, HE can occur episodically or chronically. The chosen therapy should therefore be as simple as possible to take, well tolerated and not cause any side effects.
Recent studies indicate that the composition of the intestinal flora (microbiome) also has a decisive influence on the course of various diseases. Therefore, a microbiome-gentle therapy is to be preferred. The administration of antibiotics (which are difficult to absorb) can lead to changes in the microbiome. This effect is the subject of current research.
Patients with chronic liver disease and HE often have malnutrition. They suffer from a lack of appetite, a disturbed sense of taste and a premature feeling of fullness. At the same time, they have an increased need for energy and proteins due to the disease. Deficiencies occur regardless of body weight. Overweight people with liver disease can also be affected. Active nutrition therapy is therefore sensible.
Do you think that a friend or family member might have a liver disease? Or has a friend or family member of yours recently been diagno... | more
On this page, you will find some general tips and recommendations for a healthy nutrition. Maybe not all of them apply to you – if y... | more
Hepa-Merz® contains the active ingredients L-ornithine and L-aspartate (LOLA). Both L-ornithine and L-aspartate are amino acids that ... | more